

About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。

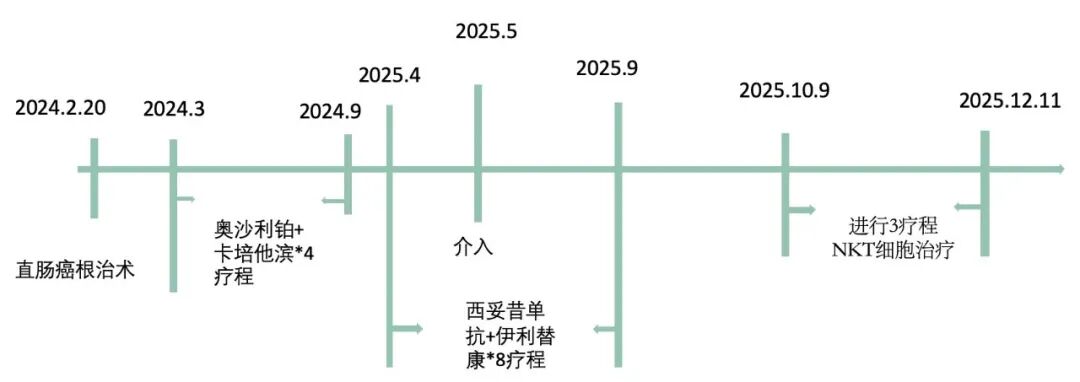
In January 2024, Mr. Li underwent a colonoscopy at a tertiary hospital in Beijing due to hematochezia, and a tumor was found approximately 12cm from the anus. Upon receiving the biopsy results, he was diagnosed with moderately differentiated adenocarcinoma of the rectum. After the diagnosis, Mr. Li's family rushed to the hospital and consulted doctors. In February 2024, he underwent radical resection for rectal cancer.
Postoperative pathology revealed a tumor with a maximum diameter of 2.5cm, involving the muscularis propria, positive vascular invasion, and lymph node metastasis (2/13), with a staging of pT2N1bMx. Immunohistochemistry showed complete expression of mismatch repair proteins, and Her-2 was negative.
After surgery, in 2024the patient entered adjuvant chemotherapy in March. Initially, the patient underwent 4courses of oxaliplatin + capecitabine, followed by 4courses of capecitabine monotherapy, until the end of 20249th month, when the chemotherapy was completed.
After the surgery to remove the tumor and undergoing 8courses of systemic chemotherapy, Mr. Li's postoperative CEA levels remained normal at around 1.7ng/ml. Mr. Li felt that the cancer cells in his body had been completely eradicated and that there should be no further issues.
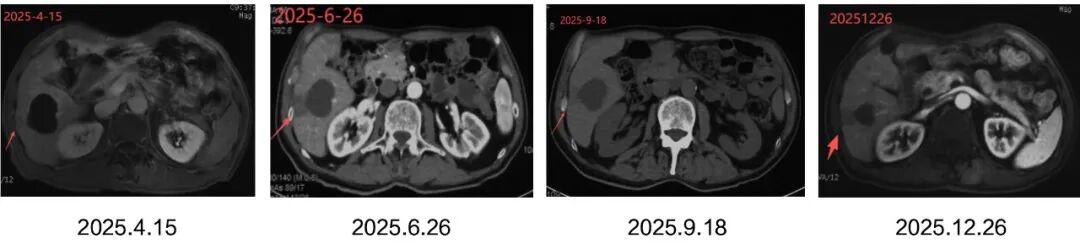
However, unexpectedly, Mr. Li's condition took a sudden turn, and a follow-up examination 13months after the surgery in March 2025revealed liver metastasis.
The liver can be said to be the favorite target organ for hematogenous metastasis of colorectal cancer. Since most of the blood from the colon and rectum flows directly to the liver via the portal vein, the sinusoidal structure of the liver slows down the blood flow, providing an opportunity for cancer cells to easily accumulate there, coupled with factors such as the suitable microenvironment for cancer cells in the liver, making the liver "preferred" by colorectal cancer.
15% to 25%of colorectal cancer patients have liver metastasis at the time of diagnosis, while another 15% to 25%of patients develop liver metastasis after radical resection of the primary colorectal cancer lesion[3].
Many people assume that cancer has reached a terminal stage and is incurable upon hearing the term "metastatic liver disease". Don't panic. For colorectal cancer, metastatic liver disease is a special case.
80% to 90% of initial liver metastases are not resectable curatively[3]. Mr. Li's situation is no exception. However, research has shown that patients with initially unresectable liver metastases can be converted to resectable or ablatable after treatment. After complete resection or ablation of liver metastases, the median survival time for patients can reach 35 to 60 months, and the overall survival rate at 5 years can reach 40% to 57%[4-8].
Therefore, in 2025year4month, Mr. Li began second-line chemotherapy, with 8courses of cetuximab+irinotecan.

During this periodin 2025year5month, microwave ablation therapy was also performed on the liver metastatic lesions.
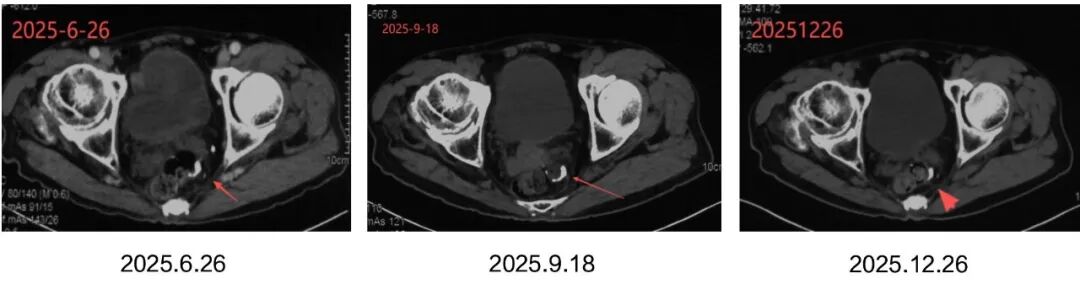
After a series of treatments, Mr. Li's tumor marker CEAbasically stabilized, and imaging showed controlled intrahepatic lesions with no new lesions. However, there was a fluctuating increase in the levels of CA19-9 and cytokeratin19 fragments.
The fluctuating increase in CA19-9 levels is often regarded as an indirect signal of intrahepatic lesion activity or progression in patients with a history of liver metastasis, as the liver is an important organ for the metabolism and clearance of CA19-9.
The fluctuating increase in cytokeratin19 fragments after treatment may reflect the activity of residual tumor cells or the presence of micro-metastatic foci. Persistent or progressive increases suggest possible disease progression.
If both indicators fluctuate and rise simultaneously, it is highly alarming, indicating the possibility of residual or early recurrent occult tumors. , Although no signs are visible on imaging, the biomarker has already shown changes.
① Systemic drug therapy: chemotherapy + targeted drugs
② Local radical treatment: minimally invasive ablation or surgery
③ Follow-up consolidation: monitoring + maintenance therapy
Mr. Li has completed steps ① and ② of treatment. Imaging examination shows that it appears "clean," but tumor markers CA19-9 and cytokeratin 19 fragments still indicate a high risk of minimal residual disease, which still makes it difficult to feel at ease.
How should we maintain the current treatment achievements, eliminate residual cancer cells, and prolong progression-free survival in the future? Surgery, chemotherapy, and radiotherapy were no longer effective. Through a friend's introduction, Mr. Li began to learn about immunotherapy techniques and ultimately chose the vNKT immune cell therapy developed by Professor Zhang Minghui's team at Tsinghua University.
✔ Mr. Li has completed systemic chemotherapy and local treatment, and currently, his tumor burden has decreased, making it the optimal window for the removal of minimal residual lesions.
✔ Mr. Li's type of intestinal cancer is almost ineffective to PD-1/PD-L1inhibitors, and traditional immunotherapy yields limited benefits.
✔ vNKT cells are a type of immune cells with both the killing power of NK cells and the specificity of T cells dual anti-tumor effects, which can not only directly kill cancer cells but also regulate the immune microenvironment within tumor tissues. They have great potential in clearing minimal residual lesions and delaying recurrence.
Experimental conditions: In the presence of vNKT cells, after 16 hours, almost all B16 tumor cells were killed!
In 2025, Mr. Li entered10months ofvNKTcelltreatment. Currently, he has completed3treatment courses, with tumor markers stabilizing and no new lesions appearing in imaging reports. His overall condition is stable.
In modern cancer treatment, being tumor-free does not equate to being risk-free. Sometimes, the invisible enemy is the most difficult to defend against. vNKT immune cell therapy is becoming an important consolidation strategy for long-term cure of cancer patients. It aims not to shrink tumors, but to prepare defenses and eliminate residual enemies before they can make a comeback. This is not only a continuation of treatment, but also an active management of long-term survival.
If you have any questions regarding post-cancer surgery immune management , you can leave a message for Professor Zhang's team.

References:
[1]Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020[J]. CA Cancer J Clin, 2020, 70(1): 7-30. DOI: 10.3322/caac.21590.
[2]Cohen R, Raeisi M, Chibaudel B, et al. Prognostic value of liver metastases in colorectal cancer treated by systemic therapy: An ARCAD pooled analysis[J]. Eur J Cancer, 2024, 207:114160. DOI: 10.1016/j.ejca.2024.114160.
[3]Vibert E, Canedo L, Adam R. Strategies to treat primary unresectable colorectal liver metastases[J]. Semin Oncol, 2005, 32(6 Suppl 8): 33-39. DOI: 10.1053/j.seminoncol.2005.07.015.
[4]de Jong MC, Pulitano C, Ribero D, et al. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multiinstitutional analysis of 1669 patients[J]. Ann Surg, 2009, 250(3):440-448. DOI: 10.1097/SLA.0b013e3181b4539b
[5]Margonis GA, Sergentanis TN, Ntanasis-Stathopoulos I, et al. Impact of Surgical Margin Width on Recurrence and Overall Survival Following R0 Hepatic Resection of Colorectal Metastases: A Systematic Review and Metaanalysis[J]. Ann Surg, 2018, 267(6): 1047-1055. DOI:10.1097/SLA.0000000000002552.
[6]Giuliante F, Ardito F, Vellone M, et al. Role of the surgeon as a variable in long-term survival after liver resection for colorectal metastases[J]. J Surg Oncol, 2009, 100(7):538-545. DOI: 10.1002/jso.21393.
[7]Padmanabhan C, Nussbaum DP, D'Angelica M. Surgical Management of Colorectal Cancer Liver Metastases[J].Surg Oncol Clin N Am, 2021, 30 (1): 1-25. DOI: 10.1016/j.soc.2020.09.002.
[8] Morris VK, Kennedy EB, Baxter NN, et al. Treatment of Metastatic Coloretal Cancer: ASCO Guideline [J]. J Clin Oncol, 2023, 41 (3): 678-700. DOI: 10.1200/JCO.22.01690.
Click to view past cases
Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com